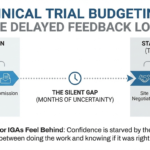
Have you ever spent a whole day building a complex, multi-arm clinical trial budget, only for a reviewer to find a glaring error in the first 30 seconds? I would argue that it is not an issue of competence, nor lack of attention to detail but a mismatch in the mode of thinking. We use different parts of our “professional brain” for the build and for the quality check (QC), and it is difficult to switch between the two on a whim.
Builder Mode – Turning Ambiguity Into Something Workable
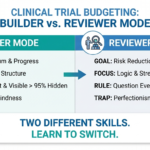
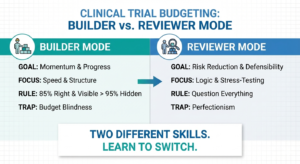
Builder mode is about translating incomplete, ambiguous information into a budget that is ready for feedback. The goal is not perfection, it is momentum. A builder’s job is to strike a balance between speed and granularity so that review, challenge, and CRO/Sponsor approval can be completed as soon as possible. At this stage, success looks like a coherent structure, reasonable assumptions, and a clear list of open questions, not a flawless end product. Over-polishing early often leads to delays, fatigue, and eventually rushed handoffs. In practice, a budget that was shared earlier and with a clear list of points to go over with your QC-er or the study team is far more useful. A budget that is 85% right and visible is more valuable than one that is 95% right and still sitting on your desktop. Done is better than perfect!
Builders are particularly susceptible to what I call “budget blindness”. After hours of working through a protocol, your brain starts seeing what you intended to do rather than what is actually in front of your eyes. That’s why, when timelines allow, stepping away matters. A few hours (or even a day, if timelines allow it), away from the build can surface issues that self-QC simply won’t catch at your initial review. Go have lunch, walk your dog, help a newer colleague with a problem they are struggling with and then come back to your budget – you will be surprised what you can discover with a fresh perspective.
Reviewer mode – Question Everything out of the Ordinary
The reviewer has a completely different goal: to stress-test decisions and look for anything that deviates from the expected. They won’t question a hematology timepoint that clearly appears in the SOA, but they will question why you applied a multiplier to ECGs at Screening.
Reviewers are usually more senior and have made the same mistakes dozens of times. They know where risk hides and go straight for it.
In reviewer mode, there is effectively zero tolerance for ambiguity or unsupported assumptions. Any question that can be asked will be asked – not to solve every open issue, but to reduce downstream rework by applying experience and best practices.
When These Two Modes Clash
Many of the same failure patterns show up repeatedly in budget QC, especially in early-stage builds.Builders should optimize for progress and momentum; reviewers optimize for risk reduction. These are different lenses applied for the same budget and trying to apply both at once leads to a substantial cognitive load. It is like trying to write an article about budget building and editing the grammar at the same time.
It is normal as a builder, to take any criticism against your work as an attack against you. It sure doesn’t help that feedback is often worded and perceived harsher than intended. Most comments are about defensibility, not intelligence, so try to separate comment from judgement. Take each criticism as a learning opportunity to identify your own shortcomings – look for patterns in feedback, not individual notes per se.
At the end of the day, we need to remember that both roles are in the same boat and have the same ultimate goal – to create a great product that needs minimal rework in the future.
How to Self-Review a Clinical Trial Budget Without Becoming Your Own Worst Enemy
Set yourself up for a mental switch – finish building first, distance yourself from your budget by doing something else for a while, then reopen the file as if you did not build it. Ask yourself:
- What was assumed and why?
- Which visits or timepoints deviate from the norm?
- If I were to review this, what would I challenge?
- What do I feel is the weakest part?
Another approach I employ is the Inversion Strategy – going through the SOA and the budget in reverse order. It helps me break the autopilot my brain goes into when reviewing something for the 11th time.
In clinical trial budgeting learning to switch between these modes is not a talent seniors are born with. It’s a skill learned the hard way, through repeated mistakes. If you feel behind, it’s because you haven’t been trained in it yet. Have a plan, externalize your steps, and keep moving forward.
Find out who I am and what I am fighting for.
If you agree, disagree, or think this is nonsense, email contact@clinicalbudget.com
If you’d like me to cover a specific topic, you can suggest it here.
Find a summary in the image below ↓

, Assumptions & CPT Codes")
")
")