One thing I did not understand when I started is why some Sponsors choose to have an additional agreement with a central lab in place, instead of just using the site’s local facility.
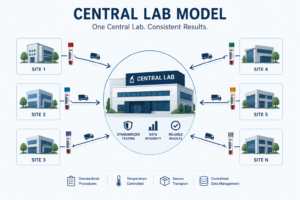
The central lab model became widely adopted in the 1980s specifically to address inconsistencies from the local-only approach, standardizing everything from lab kits and equipment to analytical methods. The emergence if this approach can be summed up in one word – consistency.
When local labs perform testing, their results will differ – they use different analytic methods, platforms, kits, and reference ranges. Central labs significantly reduce variability regardless of where the sample originated and allows for data integrity across multiple sites. This makes statistics easier to assemble and results easier to defend to regulatory agencies. Imagine a multi-country study with 80 sites – it might not be the best idea to have 80 different labs producing non-comparable hematology results they you have to defend in front of the FDA or EMA.
Central labs also offer specialized testing – genomic sequencing, biomarker testing, PK analyses that many local labs simply don’t have the equipment or expertise to run. This is especially true in oncology.
Operational downsides
While central labs improve standardization, they also introduce operational burdens at the site level. Strict collection windows, shipment cutoffs, temperature excursions, missing requisitions, or rejected samples can create significant workload and sometimes require patient recollection.
As discussed in my Central vs Local Labs article, some protocols aim to negate these negatives by allowing local labs to be performed under certain conditions/at certain visits.
How the sponsor-central lab contract works
The sponsor negotiates directly with the central lab – represented by companies like Q2 Solutions, or Fortrea (formerly Covance/Labcorp). There is an agreement that runs parallel to the budget/Clinical Trial Agreement and covers the actual cost of running the assays, managing the data, storing samples, and often arranging kit logistics and shipping infrastructure.
Sponsors select central lab providers through quality system audits, facility audits, and technical qualification for the specific procedures in the protocol. For complex global trials, they may use a full-service global central laboratory or coordinate with an umbrella CRO to manage multiple smaller regional labs.
From a budget perspective, this is why the site’s budget only captures collection and shipping – the analysis cost is already covered in a completely separate commercial agreement the site is not party to and has no visibility into. That is why including the analytical component of these tests in the site budget under a central lab model could result in double-billing the sponsor.
The site’s actual role
The site’s role is operational rather than analytical. The site collects the sample, processes it according to the lab manual specifications (centrifuge settings, temperature handling, tube type), packages it, and ships it using the courier and materials specified by the central lab, often with pre-labeled kits and dry ice already provided.
Find out who I am and what I am fighting for.
If you agree, disagree, or think this is nonsense, email contact@clinicalbudget.com
If you’d like me to cover a specific topic, you can suggest it here.