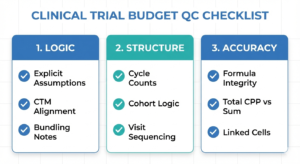
This article breaks down the most common clinical trial budget QC failure patterns and how reviewers think when flagging budgets.
Congratulations on being a budget builder! You spent hours and hours (if not days) toiling over a protocol that might seem confusing to a person without a medical background, and now it is time to be sent for review.
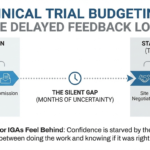
Even the most robust clinical trial budgets need to pass a round or two of quality checks (QC) – a fresh set of eyes often catches things the builder is too close to see. QC is about risk control, not perfection, and mistakes are an inevitable part of the work. I’ve seen seniors with a decade of experience miss a timepoint or overlook a nuance, so avoid taking QC comments personally.
As always, please note that your Sponsor or CRO may have requirements and specifics that are not reflected in the below guide. However, the logic behind the basics of budget building should be the same across time and space.
Missing or Unclear Assumptions: The #1 Clinical Trial Budget QC Failure
Perhaps the most important part of creating a budget from scratch is having a comprehensive list of assumptions that you made while drafting your file. Your decisions might be reasonable and robust, however, unless you have explained them in detail, the person QC-ing your file is unlikely to reach the same conclusions. It can be reasoned that you have spent more time working with the protocol than the person reviewing your work, so you are more likely to have gone through the whole thing, read all relevant footnotes and sections and noticed something that another person might miss. Perhaps you found another country budget from the same Sponsor or from the same study program and tried to mirror it for the sake of consistency, or you are familiar with this Sponsor and their specific requirements.
From the reviewer’s perspective, it is often impossible to distinguish between an error and a deliberate decision. When assumptions are not documented, even reasonable choices will be questioned.
The Golden Rule: If you are making a judgment call, make an explicit note!
Many QC issues start, at the protocol-reading stage. If you’re building budgets without a clinical background, this guide on how to read a study protocol for budgeting as a non-clinical person walks through exactly what to focus on before you ever open a budget template.
Structural Errors: When the Build Logic Breaks
Start with the study backbone (schema and arms)
The first thing I always do when looking at a protocol is finding the Study Schema and trying to figure out how many arms or cohorts this study will have – it serves as the basis of our entire budget. Get familiar and comfortable with messy flowcharts like the below and learn to filter out the noise from what actually affects your budget.
")
It might seem daunting to interpret a flowchart like that but consider the following:
- Will the participants undergo the same procedures regardless of the cohort they are assigned to?
- Is the dosing the same for all participants and will that affect the IP (investigational product) administration or drug dispensing?
- Is crossover between the different arms/cohorts allowed?
Additionally, it is a good idea to find out what the study population is – this might affect your build as well. For example pediatric studies are likely to have additional lines in their budget grid that studies with only adult populations might not.
Duration and cycles
Next, look at the Schedule of Activities (SOA) and make sure that you have a plan for how many cycles your build is going to have. The below snip is from a SOA that shows 3 cycles, with the ones after that mirroring what we have at C3:
")
Consider discussing the study duration with your Clinical Trial Manager (CTM), as they can provide useful information of what length is reasonable for the study’s population. Typically, however, the review from the CTM is the last to occur, so pick a number, add a comment that this needs to be discussed with the clinical team and move along with your build, so as to not waste time.
When going through the SOA, make sure you are consistent across procedures and arms – if items are marked as “clinically indicated”, or “at investigator’s discretion”, apply the same approach, unless you have good reason not to.
Hidden protocol details outside the SOA
Lastly, and this is something that even the most advanced budget builders may overlook, make sure to do a thorough scan of all sections of the protocol, as they may hold a nugget of information that could affect your build. Are the labs only central/local, or is there a scenario where both could be used? Are the MRI/CT scans only applicable to the areas in your SOA or does the protocol allow for other areas to be imaged? Will the prolonged infusions or the tons of PK samples require patient hospitalization? Make a note in your assumptions and raise these questions with your CTM, if needed.
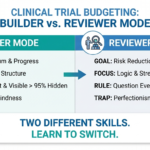
Not Thinking Like a Reviewer: Bundling and Naming Choices
It won’t do you any good if the QC-er is not aware of how or why you are combining procedures. This is one of the more complex areas of budget building, so being thorough in your assumptions will make your decisions defensible, deliberate and most of all legible. Below is what I typically do – have the name of the line, and include a list of all procedures that are related to it, instead of just having a generic name. More information is always better, as long as it is readable and relevant. Note that your site payments team will also be using your budget file, so clarity is of the utmost importance to make their job easier.
")
Related to that, I highly recommend keeping the names of procedures as they appear in your SOA. This way, even at a glance, a QC-er, a negotiator or a site will know what they are looking at. What might seem obvious to you is likely not as apparent to others.
Pro Tip: Set your budget file aside for a day. Self-QC it the next morning with a “fresh” perspective. Ask yourself, “What would I question here?”
Excel Formulas – The Last Step in a Long Journey
After making sure that you have your assumptions ready, you are certain in your structure and are ready to defend all your decisions, make sure that all of the formulas you have in your file are correct. You probably added or removed a ton of columns and rows throughout the course of your build, so don’t let a “drag and drop” error ruin your work! Check the formulas in your budget grid and ensure they are pulling the correct costs. If you dragged a formula across the whole row without locking in the cell number, it’s likely that you might have something to fix, even if the numbers seem right.
- Are the costs for the same procedures linked across the different tabs?
- Are the totals shown under each visit correct?
- Does their sum match your Total Cost per Patient?
These are all questions you need to consider before submitting your hard-won budget for review.
Over-Optimizing Accuracy: When Precision Increases Risk
One of the traps that a beginner might fall into is doing endless re-works in an attempt to be as accurate as possible. In reality, spending all of your allocated time (and there is not typically a lot of it to begin with) striving to be “perfect” is a fool errand. In a complex budget structure (i.e. one with multiple arms and tons of visits) a tiny change could have repercussions across your whole file and constant revisions can lead to more mistakes than they actually fix.
Additionally, overcomplicating something for the sake of being a tiny bit more accurate just to impress you QC-er, instead of, say, having it as invoiceable, might end up confusing your sites, local negotiators and payments teams.
Let’s take an extreme example: we have the below explanation for Vital Signs (VS) measurements, in a study where the infusion can take between 60 and 90 minutes and with overnight hospitalization:
Preinfusion, every 15 min (± 3 min) from infusion start to 1 hr post-EOI (end of infusion); every 30 min (± 5 min) during Hour 2; then every 4 hrs (± 30 min) for 24 hrs or more often, if clinically indicated.
You could do an incredibly complex calculation that takes into account how long infusions might take, if the infusion equipment monitors vitals automatically throughout the course of infusion, or if the hospitalization cost includes vitals as well…
…or you might simply mark them as invoiceable. I know what my preferred approach is. At some point, accuracy stops reducing risk and just brings follow-up questions and delays site budget approval and activation. A reviewer is not asking “Is this clever?” – they are asking “Is this defensible?” Note that I am by no means encouraging laziness or lack of effort. Cardinal decisions like that need to be discussed with your study team and I am just showing off a slightly different approach.
Passing QC consistently comes from pattern recognition and each failed attempt teaches you what to actually look for. Take the comments you receive as an opportunity to learn and try to avoid the pitfalls you have already fallen into in your next budget.
Find out who I am and what I am fighting for.
If you agree, disagree, or think this is nonsense, email contact@clinicalbudget.com
If you’d like me to cover a specific topic, you can suggest it here.
, Assumptions & CPT Codes")

")