Why does this comment sound like it is coming after me personally? Who does this guy think he is?
We have all been there – your clinical master budget comes back from a round of revisions and it is full of passive-aggressive clinical trial QC feedback, treating you like you have no idea what you’re doing. I know the feeling and I would argue that it is rarely the QC-er’s goal. The issue stems from a structural mismatch between intent, medium and mindset.
Written Comments Strip Away Tone
When a reviewer audits a budget, they aren’t thinking socially; they are focusing on the data in front of them. When I add comments, I often spew out my thoughts in a short, declarative and direct manner that aims to be as clear and outcome focused as possible.
For example: “Missing timepoint. Update” might sound more confrontational than actually is. Rarely do I go and try to soften my language or try to be diplomatic, not because I think less of a person for making a mistake. I just can’t justify delaying a deadline to add “polite padding” to twenty different comments. Short notes remove tone and intent and prioritize clarity over warmth. A comment like “Why was this marked as INV?”, that would sound neutral at worst during a call or in person, can feel accusatory on screen.
The Negativity Bias
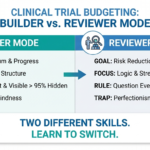
Even if 95% of your master budget is perfect, 100% of the comments you receive will point to the 5% that isn’t. You will rarely receive a “Good job!” or “Your assumptions are well thought out”. Your brain interprets clinical trial QC feedback as a comment on the quality of your performance, when it rarely is. When you are in “Builder Mode” you are an architect. You put a piece of yourself into the logic of that budget. Therefore a critique on your work feels like a critique of you as a professional and as a person.
The 15-minute Call
After each revision, I suggest setting 15 minutes aside for a quick call with your builder/reviewer and going through each comment and note. Humans are social animals and our perceptions are highly dependent on context. A perceived attack in an Excel comment can be nothing more than a person who flagged something and then simply moved on.
Actual feedback I’ve received:
Below are the comments I received for a pre-award (bid) I built after doing this job for 9 months. I thought I was infallible, I had not received even slightly negative feedback up to this point. Needless to say my fragile ego took a hit. Did it sting? Sure, but remembering this comment makes me pause and reflect about the big picture before each step.
For your continued development, below is a list of the mistakes you made
- First, note that the number of subjects involved in this study… 10,000. That means a $100 “error” on 5 visits is $500… for 10,000 subjects that is $5 million. So, we want to do all we can to make sure the bid is as accurate as possible.
- Randomization – We have this as a part of the SC fee. Is there is a reason you changed this, please let me know ASAP. This was not in your assumptions, so I had no way to know what your rationale was.
I also got the below encouragements after explaining the logic I employed and offering solutions and a way forward. They do not sound like much but they brightened up my day and showed me I was moving in the right direction.
Good approach, needs to be checked with the CTM.
A couple of good solutions, even the Emesis inclusion was a good call.
Over time, you start to see a pattern. The harshest clinical trial QC feedback often comes from people who care most about getting it right, not from those trying to score points. If you treat QC feedback as signal rather than tone, it becomes easier to extract value from it. The discomfort fades faster than the lesson.
Many of these comments stem from the same issues that appear when interpreting protocols or building assumptions into a budget. You can find a link to my “How to read a study protocol as a person with limited clinical knowledge” here.
If this list felt familiar, the Budget QC Checklist was built for exactly this situation. It walks you through every stage of the build – protocol review, site fees, cost drivers, and a final Excel check – so these mistakes don’t make it to your reviewer’s desk.
Find out who I am and what I am fighting for.
If you agree, disagree, or think this is nonsense, email contact@clinicalbudgets.com
If you’d like me to cover a specific topic, you can suggest it here.